Facebook
Facebook Google
Google GitHub
GitHub Linkedin
Linkedin
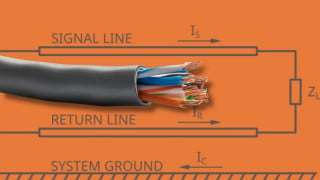
ECG leads generally see voltages in the range of -5mV to 5mV and a frequency range of .05Hz - 150Hz. We are peripherally stimulating the patients with up to 200v at a frequency of 1kHz elsewhere on the body for about 100mSec and it disrupts our front-end ECG chip. I need to protect the ECG leads from the stimulation. Although the system recovers, it takes far too long. How could we do this?
ECG EKG lead protection - TVS Diodes
- Thread starter mmarc
- Start date
-
- Tags
- diode design ecg surge